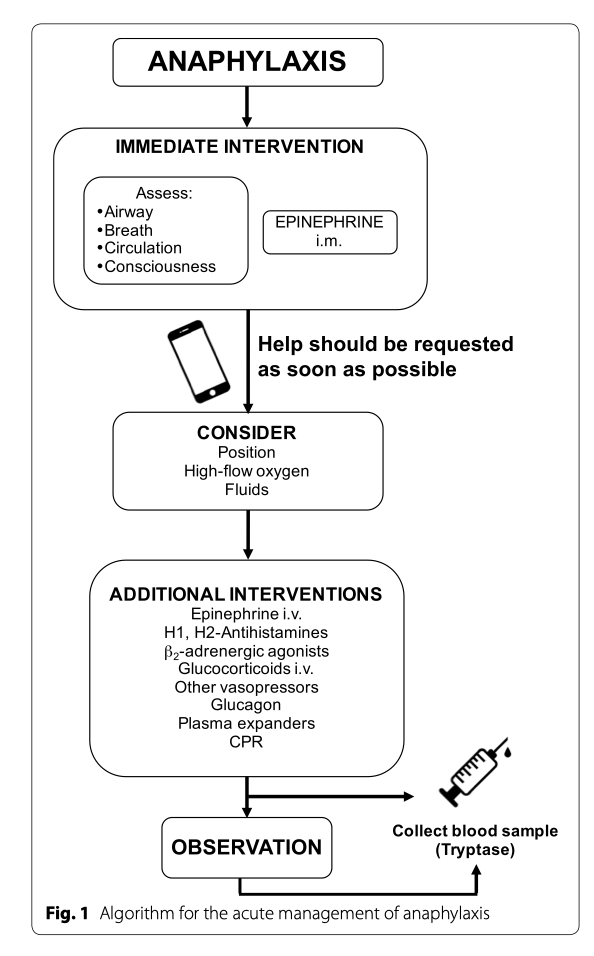
 Figure 1. Protocol for acute anaphylaxis management. From How to manage anaphylaxis in primary care, by Alvarez-Perea, Tanno & Baeza, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5724339/. Copyright 2017 by Creative Commons.
Figure 1. Protocol for acute anaphylaxis management. From How to manage anaphylaxis in primary care, by Alvarez-Perea, Tanno & Baeza, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5724339/. Copyright 2017 by Creative Commons.
Since anaphylactic reactions can be severe, quick medical attention is very important. Here are some of the things doctors and nurses might do when you arrive at the hospital.
Acute management of anaphylaxis:
Pharmacology
Potential side-effects of epinephrine:
Implications for care:
Due to the multiple systemic effects that anaphylaxis and its concurrent management manifests, it is of critical importance for healthcare staff to have the following implications for care.
Nursing Management:
Acute management of anaphylaxis:
- If you are ever experiencing an anaphylactic attack and require hospitalization, the steps the healthcare team will enact can be seen summarized in Figure 1. This includes minimizing exposure to the allergen as much as possible, as well as monitoring patient status by assessing circulation, open airway, breathing, mental status, skin, and, if possible, weight;
- Epinephrine is currently the first-line of treatment for anaphylaxis used in hospital settings and should be injected by the intramuscular route in the vastus lateralis muscle (outer thigh). Its mechanism of action as a vasoconstrictor enables it to reverse manifestations of the airway closing up and decreasing blood pressure, as well as secondary effects to the cardiac muscle and the inflammatory process;
- The intramuscular route is preferred for epinephrine as it has a vasodilator effect on skeletal muscle when administered through the intramuscular route, thus allowing for rapid absorption and onset. In contrast, if used on the subcutaneous tissue it acts as a vasoconstrictor, potentially delaying its absorption;
- After epinephrine is administered, it is best to lie on your back with your lower limbs elevated and not be placed seated, standing, or in the upright position. This should prevent distributive shock and empty vena cava/empty ventricle syndrome;
- It is crucial that help be requested as soon as possible when dealing with an anaphylactic attack. The role of nurses during patient’s care will be monitoring their vital signs (blood pressure, heart frequency, and oxygenation) continuously or as often as possible. When indicated, supplemental oxygen and intravenous fluid should be administered and, if necessary, cardiopulmonary resuscitation (CPR) could be performed (Alvarez-Perea, Tanno, & Baeza, 2017).
Pharmacology
- The dose of epinephrine for the treatment of anaphylaxis in a health centre is 0.01 mg/kg when administered intramuscularly at a 1:1000 dilution;
- The maximum dose is 0.3 mg for children and 0.5 mg for teenagers and adults;
- With an auto-injector, patients weighing between 7.5 and 25 kg should receive 0.15 mg, while patients weighing over 25 kg should receive 0.3 mg;
- The epinephrine injection can be repeated once or twice at 5–15 min intervals in patients who do not respond to the first dose, in patients whose reaction is progressing rapidly, or in a recurrent anaphylactic attack. A third dose of epinephrine is needed less frequently;
- Lack of response to epinephrine is an indicator of the need for admission to the intensive care unit, where the patient can receive further care, such as intravenous infusion of epinephrine;
- Antihistamines (both anti-H1 and anti-H2) and corticosteroids are second-line medications for the treatment of anaphylaxis, since they are not life-saving and, therefore, should not be used as initial or only treatment (Alvarez-Perea, Tanno, & Baeza, 2017).
Potential side-effects of epinephrine:
- This can include temporary anxiety, headache, dizziness, tremor, pale skin, and palpitations. However, it is important to note that these symptoms are similar to those caused physiologically by increased endogenous epinephrine levels and do not outweigh the beneficial effects of epinephrine;
- Adverse effects such as ventricular arrhythmias, pulmonary edema, malignant hypertension, and intracranial hemorrhage are seen with much fewer frequency, and are associated with too high of a dose or administration via intravenous bolus. However, this is rarely seen in children and healthy adults;
- While there is no absolute contraindication to the use of epinephrine, special considerations should be made in its use for patients with cardiovascular disease as the heart is one of the major organs to be affected during anaphylaxis (Alvarez-Perea, Tanno, & Baeza, 2017).
Implications for care:
Due to the multiple systemic effects that anaphylaxis and its concurrent management manifests, it is of critical importance for healthcare staff to have the following implications for care.
- Patient Monitoring:
- Nurses will monitor vital signs, electrocardiogram (ECG), and cardiovascular and respiratory status. Patients will be asked to report angina pain or irregular heart rate;
- To assess the effect of the medication on underlying problem (such as anaphylaxis or asthma attack), and repeat dose as needed;
- Monitor neurologic status, particularly for decreased level of consciousness and other signs and symptoms of cerebral hemorrhage or cerebrovascular accident;
- Monitor fluid intake and output, watching for urinary retention or decreased urinary output;
- Inspect injection site for infection or skin necrosis (DynaMed Plus, 2018).
- Patient Teaching:
- Teach patients who use auto-injector how to use syringe correctly, when to inject drug, and when to repeat doses;
- Inform patients that drug may cause serious adverse effects, such as palpitations, pale skin, sweating, vomiting, weakness, dizziness, headache, tremors or anxiety;
- If patients are self-administering drug outside of health care setting, explain need for prompt evaluation by a health care provider to ensure that underlying disorder has been corrected;
- As appropriate, review all other significant and life-threatening adverse reactions and interactions, especially those related to the drugs and tests mentioned above (DynaMed Plus, 2018).
Nursing Management:
- Patient positioning: Lying down on their back will help make sure the person having an anaphylactic attack is not injured if they faint, as well as help with getting rest and stabilizing blood flow. Sitting up too fast has the potential to cause complications (Alvarez-Perea, Tanno, & Baeza, 2017).
- Maintaining IV access: The person will likely have an IV placed so that if they need to be given medications quickly, or if blood has to be drawn to monitor inflammatory mediators, this can be done quickly and painlessly (DynaMed Plus, 2018).
- Airway maintenance:
- This is a critical nursing intervention as this is one of the most serious parts of an anaphylactic reaction, and without an open airway we are unable to keep breathing normally (Goodridge, Lewis, Goldsworthy, & Barry, 2014).
- This will include monitoring oxygen saturation in their blood by pulse oximetry (usually placed on their finger) and may require extra oxygen through a mask. By monitoring how much oxygen is in their blood, nurses and doctors make decisions about how much supplemental oxygen to give (DynaMed Plus, 2018).
- Ongoing assessment of how well the person is breathing is essential. The nurses and doctors will likely also prepare for more aggressive airway management, including intubation, in case the airway does not remain open and breathing becomes more compromised (Alvarez-Perea, Tanno, & Baeza, 2017).
References
Alvarez-Perea, A., Tanno, L. K., & Baeza, M. L. (2017). How to manage anaphylaxis in primary care. Clinical and Translational Allergy, 7(1), 1–10. https://doi.org/10.1186/s13601-017-0182-7
Goodridge, D., Lewis, S., Goldworthy, S., & Barry, M. (2014) Medical-Surgical Nursing in Canada: Assessment and Management of Clinical Problems (3rd Canadian Ed.). Toronto, ON: Elsevier Canada.
DynaMed Plus. (2018, Nov 30). Anaphylaxis. Ipswich, MA: EBSCO Information Services. Retrieved May 4, 2019, from http://www.dynamed.com/login.aspx?direct=true&site=DynaMed&id=113862
DynaMed Plus. (2018, Nov 30). Epinephrine. Ipswich, MA: EBSCO Information Services. Retrieved May 4, 2019, from http://www.dynamed.com/topics/dmp~AN~T908256/Epinephrine
Alvarez-Perea, A., Tanno, L. K., & Baeza, M. L. (2017). How to manage anaphylaxis in primary care. Clinical and Translational Allergy, 7(1), 1–10. https://doi.org/10.1186/s13601-017-0182-7
Goodridge, D., Lewis, S., Goldworthy, S., & Barry, M. (2014) Medical-Surgical Nursing in Canada: Assessment and Management of Clinical Problems (3rd Canadian Ed.). Toronto, ON: Elsevier Canada.
DynaMed Plus. (2018, Nov 30). Anaphylaxis. Ipswich, MA: EBSCO Information Services. Retrieved May 4, 2019, from http://www.dynamed.com/login.aspx?direct=true&site=DynaMed&id=113862
DynaMed Plus. (2018, Nov 30). Epinephrine. Ipswich, MA: EBSCO Information Services. Retrieved May 4, 2019, from http://www.dynamed.com/topics/dmp~AN~T908256/Epinephrine
